SARS-CoV-2 Causes COVID-19
Infection with the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) causes COVID-19 (COronaVIrus Disease of 2019). [1] A wide range of symptoms of COVID-19 infection appears 2 – 14 days after exposure. These symptoms include fever, cough, fatigue, headache, muscle pain, chills, sore throat, pernio-like lesions of the toes, and loss of taste or smell. While many patients are asymptomatic or have mild symptoms, other patients experience severe symptoms that can result in death. Notably, advanced age and underlying conditions are associated with higher morbidity and mortality. For example, the mortality rate is 0.2% at age 50, 0.75% at age 60, and 27% for ages 85 and above. [2]
Viral Entry
The SARS-CoV-2 Spike (S) protein, which is the principal structural protein on the outside of the viral particle, is necessary for viral entry into host cells (Figure 1). [3] As such, the S protein is of particular interest to the research community. The S protein is 1273 amino acids in length and comprised of two extracellular subunits (S1, S2).
The first step in viral entry is the interaction between the S protein – via its receptor-binding domain (RBD) – and the host’s angiotensin-converting enzyme (ACE2) receptor. Subsequently, the host’s type II transmembrane protease (TMPRSS2) cleaves the S protein twice: once between the S1 and S2 subunits and once within the S2 subunit. This crucial cleavage step is known as priming, which allows the fusion of the S-protein with the cell membrane. Other host receptors, including neuropilin-1 (NRP1) and tyrosine-protein kinase receptor UFO (AXL), also facilitate viral entry. [4,5] Inside the cell, the virus hijacks host cell transcription to replicate more of itself. Finally, mature virions are released to infect other cells.
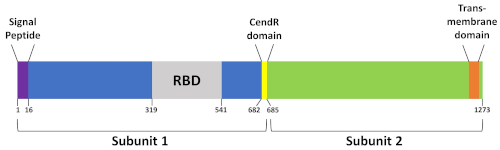
Figure 1. SARS-CoV-2 Spike protein domains. Spike proteins have two subunits (S1, S2). Located within the S1 subunit., the receptor binding domain (RBD) can bind to ACE2 and the CendR domain can bind to NRP1. The numbers below the domains show the amino acid position.
Neutralizing Assays
The ability to “neutralize” the Spike-ACE2 interaction could be an effective method to prevent and treat COVID-19. For example, both vaccines that have been approved by the U.S. Food and Drug Administration (FDA) stimulate the immune system to produce antibodies to the S protein. [6] Neutralization assays that measure a molecule’s ability to inhibit the formation of the S-ACE2 complex are used to screen patient serum for neutralizing antibodies, validate inhibitors of the S-ACE2 interaction, and develop COVID-19 vaccines.
In vitro binding assays generally immobilize the S protein or ACE2 onto a solid substrate, such as a 96-well plate, and then probe with the ACE2 or S protein (“probe”), respectively, in the presence of a potential inhibitor. The S-ACE2 interaction is then detected using an anti-probe antibody labeled with horseradish peroxidase (HRP), which produces a blue color in the presence of TMB that is proportional to the amount of S-ACE2 complex. The HRP-TMB reaction is stopped with sulfuric acid, resulting in a blue-to-yellow color change. The intensity of the yellow color is then measured at 450 nm. Successful inhibition of the S-ACE2 interaction is reflected when the optical density (OD) with the inhibitor is lower than the OD without the inhibitor (i.e., only S + ACE2).
In Figure 2, two plasma samples from COVID-19 patients were collected 30 days post symptom onset and analyzed with the RayBio® Spike-ACE2 Binding Assay Kit (cat no. CoV-ACE2S2). Plasma diluted at 1:20 and 1:125 from Patient A inhibited the S-ACE2 interaction 88% and 52%, respectively when compared to the “no sample” positive control. A higher amount of plasma resulted in higher inhibition, reflecting a titration-dependent response. In comparison, the S-ACE2 interaction was minimally inhibited by Patient B serum at both dilutions. These data reveal that Patient A’s immune system produced neutralizing antibodies in response to COVID-19 infection whereas Patient B did not. Plasma from COVID-19 patients that contain neutralizing antibodies – or antibodies that inhibit viral infection – may also prove to be effective convalescent plasma therapy (i.e., plasma transfusion) to treat COVID-19. [7,8] Such therapy is considered investigational.
Plate-based in vitro binding assays are rapid (< 1 day), simple to use, and require a common laboratory instrument (i.e., plate-based reader). Furthermore, they offer a safer alternative compared to working with a live virus (biosafety level 3) and a more affordable option compared to working with pseudoviruses that require multiple plasmids and cell lines (biosafety level 2). Finally, in vitro binding assays such as RayBiotech’s COVID-19 Spike-ACE2 Binding Assay Kits (cat no. CoV-SACE2, CoV-ACE2S2) enable the high throughput screening of hundreds to thousands of different molecules simultaneously. These molecules could include small molecules, peptides, proteins, aptamers, or antibodies. Similar plate-based assays can also be employed to screen potential inhibitors of Spike interactions with other important endogenous receptors, NRP1 and AXL (cat no. CoV-NRP1S1, CoV-SAXL). [4,5] Identification of molecules capable of inhibiting the S protein’s interactions with relevant endogenous receptors in vitro can be further investigated using cell-based assays and, eventually, within clinical trials.

Figure 2. Measurement of COVID-19 patient plasma with an in vitro binding assay. Patient plasma was diluted at 1:20 and 1:125 and analyzed with the RayBio® Spike-ACE2 Binding Assay Kit (cat no. CoV-ACE2S2). Error bars represent triplicate analyses.
SARS-CoV-2 Pseudovirus
Neutralization methods that use live SARS-CoV-2 require working under strict bio-containment conditions in biosafety level-3 (BSL-3) laboratories. These types of facilities are rare and expensive to operate. A more affordable, safe, and accessible option is a SARS-CoV-2 pseudovirus, which is a viral particle that can mimic viral entry and replicate only once. [9] Because of this, the pseudovirus can be handled at BSL2.
Like the active virus, the SARS-CoV-2 pseudovirus expresses the S-protein on its surface. A plasmid encoding for luciferase is contained inside the pseudovirus particle; no other nucleic acid is present inside the pseudovirus. When the pseudovirus is incubated with ACE2-expressing cells, the S-protein binds to the ACE2 receptor. The membranes of the viral particle and cell then fuse, causing the plasmid to be released into the host cell where luciferase will be expressed. Upon addition of a luciferase substrate, cells that have been successfully infected with the pseudovirus luminescence. In the presence of molecules (e.g., small molecules, peptides, antibodies) that neutralize the S-ACE2 interaction, the luminescence decrease. The inhibition rate of the molecule can be determined by comparing the amount of luminescence when the molecule is added to the amount of luminescence when the molecule is not added.
In the example provided in Figure 3, plasma from various patients were analyzed using the SARS-CoV-2 pseudovirus. Patient C’s plasma was obtained before the COVID-19 outbreak. Therefore, Patient C’s plasma does not contain any antibodies to SARS-CoV-2 and no neutralizing activity was observed with the pseudovirus assay. Plasma samples collected 42 days after symptom onset were collected from two patients (Patients D, E). While plasma from both patients inhibited pseudoviral entry, plasma from Patient D was more effective than plasma from Patient E. Like Patient D, plasma from Patient F also had significant neutralizing activity. However, unlike Patient D who had been diagnosed with COVID-19, Patient F had completed both doses of the FDA-approved COVID-19 vaccine from Moderna 42 days prior to sample collection.
Researchers who do not have the resources to perform a neutralization assay with a SARS-CoV-2 pseudovirus can send their potential S-ACE2 inhibitors for analysis using RayBiotech’s COVID-19 Pseudovirus Service.

Figure 3. Measurement of patient plasma with a SARS-CoV-2 pseudovirus assay. Plasma samples from a non-COVID-19 patient (Patient C), COVID-19 patients (Patients D and E; 42 days post symptom onset), and vaccinated patient (Patient E; 42 days after completing a COVID-19 vaccine series) were diluted at 1:50, 1:100, and 1:200.
Conclusions
The SARS-CoV-2 Spike protein plays a critical role in viral entry and, as such, is an important target in COVID-19 vaccine and drug development. In vitro binding assays and the SARS-CoV-2 pseudovirus assay can help screen potential “neutralizing” inhibitors of viral entry. Although not discussed in this article, cell-based ELISAs, biolayer interferometry, and flow cytometry can also be used to study the S-ACE2 interaction in the presence of potential inhibitors. [10,11] Focus reduction neutralization tests (FRNT) or plaque reduction neutralization tests (PRNT) with live SARS-CoV-2 virus can measure SARS-CoV-2 infectivity in the presence of potential viral inhibitors. [12]
References
- He F, et al. Coronavirus disease 2019: What we know? J Med Virol. 2020 Mar 14.
- Levin A, et al. Assessing the age specificity of infection fatality rates for COVID-19: systematic review, meta-analysis, and public policy implications. medRxiv. 2020 2020.07.23.20160895.
- Hoffmann K, et al. SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell (2020).
- Cantuti-Castelvetri L, et al. Neuropilin-1 facilitates SARS-CoV-2 cell entry and infectivity. Science. 370, 865-860 (2020).
- Daly JL, et al. Neuropilin-1 is a host factor for SARS-CoV-2 infection. Science. 370, 861-865 (2020).
- Dai L and Gao GF. Viral targets for vaccines against COVID-19. Nature Reviews Immunology 21, 73-82(2021).
- Zhang B, et al. Treatment with convalescent plasma for critically ill patients with severe acute respiratory syndrome coronavirus 2 infection. Chest. 2020 Mar 31;S0012-3692(20)30571-7
- Pawar AY, et al. Convalescent plasma: a possible treatment protocol for COVID-19 patients suffering from diabetes or underlying liver diseases. Diabetes Metab Syndr. 2020 July-August; 14(4): 665–669.
- Whitt M. Generation of VSV pseudotypes using recombinant ΔG-VSV for studies on virus entry, identification of entry inhibitors, and immune responses to vaccines. J Virol Methods. 2010 Nov;169(2):365-74.
- He Y, et al. Receptor-Binding Domain of Severe Acute Respiratory Syndrome Coronavirus Spike Protein Contains Multiple Conformation-Dependent Epitopes that Induce Highly Potent Neutralizing Antibodies. J Immunol. April 15, 2005, 174 (8) 4908-4915.
- Zhang G, et al. The first-in-class peptide binding to the SARS-CoV-2 spike protein. bioRxiv https://doi.org/10.1101/2020.03.19.999318
- Suthar MS, et al. Rapid Generation of Neutralizing Antibody Responses in COVID-19 Patients. Cell Rep Med. 2020 Jun 23; 1(3): 100040.