
By Rafael Rosengarten, Ph.D., Chief Executive Officer, Genialis
The inclusion of a biomarker in the design of clinical trials has been found to increase the odds of meeting the trial endpoint and advancing to the next stage of development by 5-12x in the top five most prevalent cancers.1
Yet, most approved biomarkers for predicting treatment response or benefit fall short of the hopes and expectations of drug developers, doctors and patients.
In this article, we will explore the potential of RNA biomarkers in precision medicine. Before delving into the intricacies of RNA biomarkers, let's first understand what biomarkers are and how they have revolutionized the field of medicine.
- What is a Biomarker?
- The Current State of Biomarker Applications
- The Need for Better Biomarkers
- The Challenges of Traditionally Used Biomarkers
- DNA-based Biomarkers
- Protein-based Biomarkers
- The Journey Towards RNA Biomarkers and Their Advantages
- The Impact of RNA Biomarkers in Cancer Care
- Machine learning behind the success of RNA biomarkers
What is a Biomarker?
A biomarker, short for "biological marker," is any measurable indicator of some biological state or condition. Biomarkers are characteristics that offer insights into normal or pathological processes or responses to a therapeutic intervention.
Identifying biomarkers is especially useful in the realm of cancer, where they have been nothing short of revolutionary in some disease histologies and for guiding certain medicines. Biomarkers have paved the way for early detection, diagnosis, risk assessment, and the tailoring of treatment plans to individual patients' needs. Famous examples include EGFR mutation status in lung cancer and the indication of tyrosine kinase inhibitors2, and BRAF V600E and its indication of vemurafenib which totally upended the treatment of melanoma.3
The Current State of Biomarker Applications
More specifically, biomarkers have impacted the field of oncology in:
- screening (e.g. CA-125 in ovarian cancer),
- diagnosis (e.g. KRAS G12C alteration in non-small cell lung cancer),
- choice of treatment (e.g. a tyrosine kinase inhibitor for an EGFR exon 19 deletion in non-small cell lung cancer as a first-line treatment versus chemotherapy) and
- prediction (e.g. BRCA1, BRCA2 status in inherited breast cancer).
While biomarkers changed the way we view and treat cancer, their success in predicting drug efficacy still hasn’t reached its full potential. Why is that?
The Need for Better Biomarkers
Let’s take a look at the data and an instructive example.
As of 2020, roughly 27% of cancer patients were eligible for genome-informed therapy, while only 11% of cancer patients showed a clinically beneficial response to such treatment. Meanwhile, the durability of response has been stagnant at ~18 months for nearly the past two decades.4
PD-L1 is a valuable prognostic biomarker for overall survival across a variety of cancers.5 It has also been approved by the FDA as a companion diagnostic for immune checkpoint therapy.
However, a retrospective study of all clinical trials between 2011 and 2019 prompting FDA approval of immune checkpoint inhibitors identified PD-L1 as a predictive biomarker in only about 30% of cases.6 Better biomarkers are required.
The Challenges of Traditional Biomarkers
The first choice to make is what to measure as a readout of the disease in order to guide therapeutic decision-making.
DNA and RNA are molecules that form the basis of every cell and are precursors to the formation of proteins that make up the human body, and all three may be analytes that serve as biomarkers associated with various aspects of health and disease.
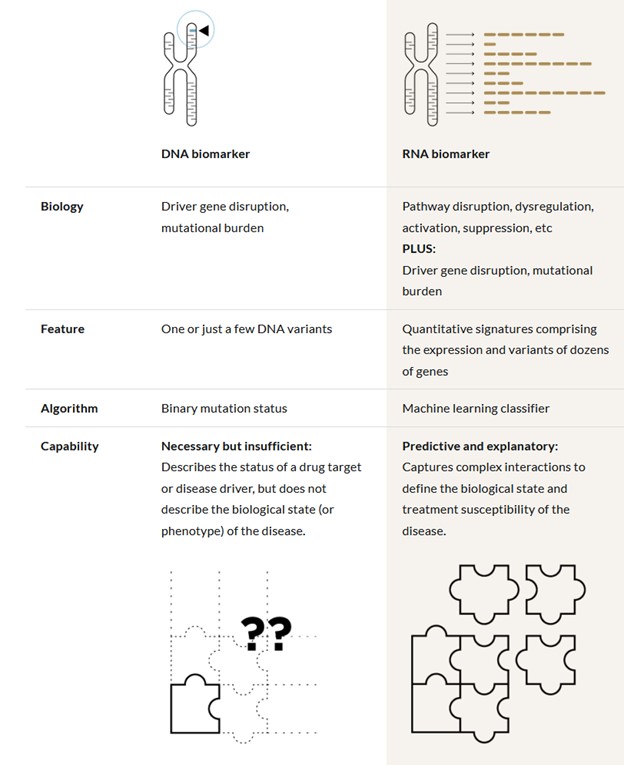
DNA-based biomarkers
- Common Use: Predominantly employed for predictive biomarker discovery and companion diagnostics.
- Examples:
- EGFR T790M mutations in metastatic non-small cell lung cancer: Guides the use of osimertinib for resistance to first-generation tyrosine kinase inhibitors like erlotinib.
- KRAS G12C mutations
- Limitations: While DNA reveals genetic predispositions and mutational statuses, it falls short in reporting cellular phenotypes—that is, the physiological status of the tumor and tumor milieu— associated with disease onset or progression.
Protein-Based Biomarkers
- Therapeutic Targets: Proteins often serve directly as targets (e.g., HER2 levels in breast cancer and subsequent treatment with Trastuzumab).
- Variety: Can include cancer antigens (like CEA), enzymes, hormones, or unique protein modifications (e.g., distinct glycosylation profiles in tumors).
- Techniques: Relies on ELISA, mass spectrometry, or immunohistochemistry.
- Challenges:
- Reproducibility Issues: Variability in antibody-based methods across labs.
- Complexity and Cost: Particularly for mass spectrometry.
- Masking Effect: Dominantly expressed normal proteins can obscure cancer-specific proteins or modifications.
The Journey Towards RNA Biomarkers
Despite the pivotal role of traditional DNA and protein-based biomarkers, these have limitations that minimize their effectiveness in improving patient outcomes. They can identify genetic mutations or express proteins associated with cancer but often fail to capture the dynamic changes occurring within cells that influence disease progression and response to treatments.
This search for more effective biomarkers brings us to RNA.
Gene expression-based biomarkers provide dynamic insights into cellular states and regulatory processes when compared with DNA or protein biomarkers. These aspects of disease biology are especially relevant to predicting treatment outcomes of complex diseases.
Advantages of RNA-based Biomarkers
- Dynamic Snapshot of Cellular Activity
- Key Insight: RNA provides a real-time picture of cellular physiology, showcasing active biological states.
- Why It Matters: RNA reports gene expression tied to disease progression, responses to drugs, or other stimuli, offering a deeper understanding than DNA's static readout.
- Mutation Insights Through Expression
- Key Insight: Just like DNA, mutation status can be inferred from RNA, while RNA also provides quantitative measurements of gene expression.
- Why It Matters: Incorporating mutation status with gene expression allows multi-modal interpretation, which can refine a biomarker’s capabilities for patient selection and treatment outcome prediction.
- The Wealth of Data in RNA Sequencing
- Key Insight: Total RNA sequencing captures a wide array of RNA types, both protein-coding (mRNA) and non-coding (miRNA, lncRNA), enriching our understanding of cancer biology.
- Why It Matters: Gene expression can encompass the entire genome’s worth of activity, providing a high dimensional data-scape from which to understand tumor biology. The information encoded in RNA helps unravel complex interactions and regulatory mechanisms at play in cancer, providing a nuanced view beyond DNA's capabilities.
Common concerns regarding RNA-Seq include its cost, access to bio-specimen material, and data reproducibility. Given advancements in the state of the art, RNA-Seq has become more attractive as a clinical analyte as some of the above objections are satisfied.
The ability to multiplex many different tests from the same analyte combined with the ever-decreasing costs of sequencing makes transcriptomic biomarkers cost-effective for complex disease diagnosis, and clinical R&D. As RNA-seq gains popularity, Genialis has assisted the bioinformatics community in selecting the appropriate normalization method for RNA-seq data.
The Impact of RNA Biomarkers in Cancer Care
The practical applications of RNA biomarkers in oncology are vast and varied. From enhancing the accuracy of early cancer detection to refining the selection of therapeutic targets, RNA biomarkers are set to transform how we approach cancer treatment.
Recent developments have highlighted the potential of RNA-based biomarkers in enhancing the effectiveness of cancer treatments across various mechanisms of action (MOA) and tissues of origin. One example of this progress is the creation of the XernaTM TME Panel, which was developed to predict response to virtually any drug targeting the tumor microenvironment (TME), and has been shown to enrich for clinical benefit to numerous approved and investigational drugs across a dozen solid tumors.7,8
Another recent example is the biomarker GenialisTM krasID, which uses RNA-sequencing to predict response and benefit to the emerging class of KRAS inhibitors. Mutation screening alone for KRAS G12C mutations in non-small cell lung cancer (NSCLC) lead to 30-40% patient response rates and 6–11-month durability of response. The krasID biomarker can predict with >80% accuracy real world patient response to sotorasib and can definitely stratify patients based on high and low duration of benefit.9
RNA Biomarkers: Bridging the Gap in Diagnostic Innovations
To date, the diagnostic potential of RNA as an analyte has been underexplored. However, regulatory bodies are increasingly recognizing the value of RNA biomarkers. Efforts are underway to integrate such biomarkers into clinical applications, including assays for clinical trials, research tools, and companion diagnostics for specific therapies.
For example, Xerna TME Panel is currently being developed for clinical applications as a clinical trial assay with FDA IDE acceptance; an LDT for clinical research; and as a CDx for a novel anti-angiogenic drug.
Machine learning behind the success of RNA biomarkers
The success behind the recent advancements in RNA-based biomarker technology is rooted in the implementation of novel machine learning techniques. These techniques are designed to ensure that biomarker models are universally applicable across various clinical contexts and hold up in real-world scenarios.
Here's a closer look at some of the important considerations in the process:
- Selective Gene Inclusion: It’s important to employ methods that select only those genes that are consistently and robustly expressed across different bias modalities, such as tissue types and platforms, to be included in the predictive model.
- For example, the Xerna TME panel comprises approximately 100 genes that performed consistently in data derived from numerous cancer types generated by various sequencing providers, each with a different protocol and platform.
- Mitigating Variability: The comprehensive nature of the panel's genetic signature has to ensure redundancy in the signals it detects. This redundancy is crucial for counteracting the potential impact of both technical and biological variability, leading to more stable and reliable model performance.
- The end product should be a reproducible and robust RNA-based biomarker that predicts clinical benefit in the real world.
CONCLUSION
While RNA has historically been underutilized as an analyte for diagnostic devices, regulatory bodies have demonstrated a keen interest in this class of biomarkers. RNA-based biomarkers will be game-changing. Drug developers should adopt these predictive biomarkers now to increase cost-effectiveness, offer better diagnostic and therapeutic options, and ultimately improve patient outcomes.
Sources
[1] Parker JL, Kuzulugil SS, Pereverzev K, et al. Does biomarker use in oncology improve clinical trial failure risk? A large-scale analysis. Cancer Med. 2021;10(6):1955-1963. doi:10.1002/cam4.3732
2 https://www.cancer.org/cancer/types/lung-cancer/treating-non-small-cell/targeted-therapies.html
3 McArthur et al. Safety and efficacy of vemurafenib in BRAF(V600E) and BRAF(V600K) mutation-positive melanoma (BRIM-3): extended follow-up of a phase 3, randomised, open-label study. Lancet Oncol. 2014 Mar;15(3):323-32. doi: 10.1016/S1470-2045(14)70012-9.
4 Haslam A, Kim MS, Prasad V. Updated estimates of eligibility for and response to genome-targeted oncology drugs among US cancer patients, 2006-2020. Ann Oncol. 2021;32(7):926-932. doi:10.1016/j.annonc.2021.04.003
5 Mok TSK, Wu YL, Kudaba I, et al. Pembrolizumab versus chemotherapy for previously untreated, PD-L1-expressing, locally advanced or metastatic non-small-cell lung cancer (KEYNOTE-042): a randomised, open-label, controlled, phase 3 trial. Lancet. 2019;393(10183):1819-1830. doi:10.1016/S0140-6736(18)32409-7
6 Davis AA, Patel VG. The role of PD-L1 expression as a predictive biomarker: an analysis of all US Food and Drug Administration (FDA) approvals of immune checkpoint inhibitors. J Immunother Cancer. 2019;7(1):278. Published 2019 Oct 26. doi:10.1186/s40425-019-0768-9
7 Fu S, Corr BR, Culm-Merdek K, et al. Phase Ib Study of Navicixizumab Plus Paclitaxel in Patients With Platinum-Resistant Ovarian, Primary Peritoneal, or Fallopian Tube Cancer. J Clin Oncol. 2022;40(23):2568-2577. doi:10.1200/JCO.21.01801
8 Uhlik M, Pointing D, Iyer S, et al. Xerna™ TME Panel is a machine learning-based transcriptomic biomarker designed to predict therapeutic response in multiple cancers. Front Oncol. 2023;13:1158345. Published 2023 May 12. doi:10.3389/fonc.2023.1158345
9 Žiberna K, Lovše A, Vohar L, et al. Biology-Driven Machine Learning to Personalize KRAS Inhibitor Therapy. AACR 2024.