Featured Article

Laboratory information systems must take a page out of the manufacturing playbook
Most health-care enterprises think of their laboratory information system (LIS) as a clinical information system that receives, processes, and stores information from diagnostic tests. In reality, while the laboratory produces a clinical product, the high-volume laboratory data work flow is fundamentally different from the clinical data work flow. More closely akin to what a manufacturing environment delivers, laboratory information systems must work with a minimum of variation and a higher degree of accuracy than clinical information systems.
The sheer number of tests done and the widespread use of automated robotic lines to help laboratories work through the volume to deliver a product with minimal variation and high degrees of accuracy makes the manufacturing analogy particularly apt. Modern hospital-based laboratories have also been enthusiastic adopters of lean manufacturing processes, in another nod to the manufacturing paradigm.
Most health-care electronic medical record (EMR) systems include a module for clinical laboratory information technology, based on the underlying assumption that the LIS is simply a module of the larger clinical information system. But is it? Or, does the high-volume, high-stakes, factory-like laboratory work flow separate the LIS from the rest of the EMR, requiring a more robust system that can drive improvements in patient safety, increase revenue by reducing turnaround time, and meet interoperability standards required under meaningful use criteria?
Continuing the manufacturing analogy, many modern manufacturing processes use what is known as an enterprise resource planning (ERP) system to link all departments and functions across a company onto a single system. In the classic manufacturing assembly line context, an ERP system links materials management, production management, sales and order management, financial management, customer relationship management, and services and support, among others.
To support the laboratory work flow, the LIS should actually serve a similar function. Rather than an enterprise resource planning system, it might be referred to as a laboratory resources planning (LRP) system. An LIS that is an LRP would contain tools to manage specimens, staff, and all other laboratory resources. It would also have business intelligence and analytics that guide organizations to make data-driven decisions affecting such processes as time and attendance, productivity, quality assurance, critical results, and infectious disease surveillance.
Laboratory work flow is at the heart of health-care decisions
The hospital laboratory work flow is far different from that of any other area of the hospital. Laboratory records associated with managing a specimen once it has been obtained are very different from records developed to document patient care, derive a diagnosis, monitor the treatment plan, or administer medication.
In effect, laboratory test results should be thought of as a clinical product that is the result of a manufacturing work flow. Laboratory work flow utilizes several controls that are manufacturing-related, including quality assurance/quality control steps and validation, among others. Analogous to a factory, in which large volumes must be managed with a high degree of accuracy and reliability, hospitals process millions of samples to produce clinically accurate and appropriate results per year.
In addition, laboratory results are a critical part of the health-care process. While laboratory tests make up only about 2.3 cents of every dollar spent on health care, laboratory test results data account for approximately 70% of patients’ medical records, and affect between 70 and 80% of the clinical decisions made. Sophisticated use of information technology enhances the value of these laboratory test data.
The combination of such a high volume and the diagnostic value of the information means that hospitals can ill afford any kind of hiccups in their system. It also means that it is absolutely critical that the LIS have the capability to communicate accurate, reliable laboratory results to care providers who make decisions.
In fact, this very communication is at the heart of initiatives to reduce medical errors and reduce health-care costs, and is key to receiving incentives for meeting meaningful use objectives under the Health Information Technology for Economic and Clinical Health Act (HITECH Act). Interoperability among data systems is a key theme throughout the meaningful use definition.
The meaningful use criteria require electronically capturing health information in a standard format, using that information to track key clinical conditions, communicating the information for care coordination purposes, and initiating the reporting of clinical quality measures and public health information.
Laboratory volume and utilization central to future of health care

Figure 1 - Growth of laboratory test volume and utilization.
As shown in Figure 1, laboratory test volume and utilization has been growing, driven largely by demographic trends as the baby boom generation ages. Centers for Medicare & Medicaid Services (CMS) data suggest that, prior to age 65, patients utilize an average of two laboratory tests per year, while after age 65, this number climbs to about nine tests per year. Other trends driving the increase include the evolution in personalized medicine and the growing array of esoteric tests, technology advances in early diagnosis and treatment, and an increased focus on prevention and wellness.
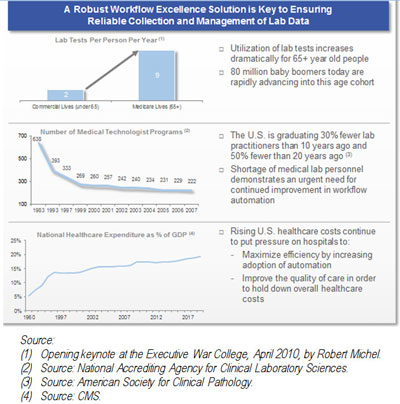
Figure 2 - Ttrends in test volumes and medical technician and related programs.
In recent years, as test volumes rose due to demographic and other trends, medical technician and related programs actually decreased, creating the demand for technology to help hospitals improve handling of large volumes with fewer staff. Figure 2 illustrates these trends graphically. The mismatch between the growth in tests done and the number of technicians available to conduct laboratory analyses has resulted in a situation in which the huge volume increases have required automated robotic lines to help technicians work through the volume with minimal variation and a high rate of predictability.
Patient safety is one of the nation’s most pressing health-care challenges, and numerous studies show the potential for patient harm in the specimen labeling process. One study found that 1 in 18 sample identification errors leads directly to an adverse event.1 Another study found that a surprising 5.8% of phlebotomy samples are mislabeled.2

Figure 3 - Automated robotic lines.
Automated robotic lines, shown in Figure 3, illustrate the modern manufacturing work flow that must be central to improving the sample work flow and increasing patient safety. In addition, new lean work flow initiatives, incorporating lean manufacturing processes at the bedside, are also being brought in to improve the accuracy in these highly variable processes.
Increasing productivity delivers improved return-on-investment (ROI)
A best-of-breed LIS can be used to increase productivity for the estimated 40% of tests performed by hospital-based laboratories on outreach or outpatient specimens. These samples, sent in by ambulatory or community-based facilities such as physicians’ offices, contain a bar-code label from their EMR, usually accompanied by an additional paper copy of the order. Because the bar-code label is unfamiliar to the LIS, the order is manually entered into the LIS, a new label is generated, and the sample is relabeled with a bar code that can be consumed by the LIS.

Figure 4 - Rise in revenue as a result of increasing laboratory capacity.
Advanced laboratory information solutions make it possible for laboratories to receive foreign specimens without having to relabel them. Such systems have the ability to route samples through the laboratory, and determine which analyzer will be used, and even which rack the sample will be temporarily stored in. This can eliminate variation, speed up the process, and subsequently create additional capacity. These advanced LIS-delivered work-flow automation solutions lessen the possibility of errors resulting from the relabeling process, and create expanded capacity that will provide opportunities to drive additional profitable revenue. Figure 4 provides an example of the revenue increases made possible by eliminating the need to relabel samples with foreign bar-code identifiers.

Figure 5 - Example of diagnostic intelligence helping to ensure data-driven decisions.
In addition to increasing productivity, the LIS should have the ability to use data in real time to help manage the business by guiding organizations to make data-driven decisions, increase organizational transparency, and improve patient safety. Business intelligence and analytics tools provide accurate diagnostic key performance indicator (KPI) management and the ability to measure cost reductions through improved operations, real-time alerts, and the proactive identification of trends. Figure 5 shows a sample of the kinds of data that laboratories should have access to.
Conclusion
Laboratory work flow is unique within health care. It offers a clinical product in which extremely high volumes must be delivered with a high degree of accuracy. Automation is the key to the efficient work flow needed, and is an important element in achieving meaningful use goals. The importance of accurate, reliable results in the face of this high-volume demand cannot be overstated.
The LIS is evolving to deliver increased functionality to the entire health-care enterprise. ROI for the LIS is measurable and repeatable, and helps articulate the laboratory service line’s objective value to the enterprise. Along with patient safety, increased capacity, and interoperability, business intelligence analytics and metrics must be part of the LIS, a key to effective data-driven management.
In the competitive health-care market, rather than simply serve as a module within an EMR system, the LIS must act as a resource planning tool, driving improvements in patient safety, increasing revenue by reducing turnaround time, and meeting interoperability standards required under meaningful use criteria.
References
-
Valenstein, P.N.; Raab, S.S.; Walsh, M.K. Identification Errors Involving Clinical Laboratories: A College of American Pathologists Q-Probes Study of Patient and Specimen Identification Errors at 120 Institutions. Archives of Pathology & Laboratory Medicine; Aug 2006, Vol. 130, No. 8, pp. 1106–1113.
- Lippi, G.; Salvagno, G.L. et al. Phlebotomy issues and quality improvement in results of laboratory testing. Clin. Lab. 2006, 5+6.
Ms. Feist is Vice President of Marketing, Sunquest Information Systems, 250 South Williams Blvd., Tucson, AZ 85711, U.S.A.; tel.: 520-570-2000; e-mail: [email protected].